
Have you recently had an imaging exam such as an X-ray, ultrasound, nuclear medicine scan, CT scan, or MRI scan but find yourself struggling to understand what your radiologist is saying in your radiology report?
You might wonder, “What is a radiology report?” and “Why is it important for me to understand it?” Let’s unravel this together!
Radiology and Its Place in Your Healthcare
Let’s start with a bit of background on medical imaging and radiology as they’re infrequently featured on TV shows 😉 (Though feel free to skip to The Radiology Report section below.)
What is Medical Imaging?
Medical imaging is a continuously evolving, powerful tool often used to aid in diagnosing innumerable medical conditions, screen for various cancers, and significantly guide and impact patient care.
Think of diagnosis as the first step in solving a health mystery. When you’re not feeling right or have certain symptoms, doctors use imaging to look inside your body and gather clues. Just like a mechanic peeks under the hood to see what’s going on with a car, medical imaging lets doctors see what might be causing your health issues. It’s a way to pinpoint the problem so they know what to treat and how to treat it.
Example: Appendicitis, enteritis (inflammation or infection of the GI tract), kidney stone, ruptured ovarian cyst, and more can all cause right lower quadrant abdominal pain but are managed VERY differently, ranging from emergent surgery to reassurance.
While figuring out health mysteries is a key reason for medical imaging, it’s not the only one. Here are some other important reasons why you might get an image taken:
- For Preventive Care: Diagnosing treatable conditions before they cause symptoms allows you to take early action and minimize negative effects on your health. If you’re at risk for certain conditions, a peek inside can help catch any issues early on, which is often when they’re easier to treat. This primarily consists of screening tests (lung cancer screening CT, calcium score CT for coronary artery disease screening, CT colonography for colon cancer screening, mammography for breast cancer screening, liver ultrasound for liver cancer screening, etc.) performed in at risk individuals. The goal: catch cancers early when they’re easier to treat or even curable.
- To Guide Treatment: Radiology plays a critical role in guiding the management of many cancers. It helps determine if surgery is an option, which surgical approach is most appropriate, or if the cancer has (unfortunately) already spread to other parts of the body (metastasized). Imaging findings can also guide surgeries and procedures, from having a knee replaced, a gastric bypass, an aortic valve placed by a minimally invasive technique, or even intraoperative guidance during brain surgery.
- To Monitor a Condition: A thorough medical examination (questions, physical exam, and blood work) can only give so much information. Some conditions require imaging for monitoring, such as cancer status (to see if a new treatment regimen is working or confirm a person’s cancer is still in remission), presence of small bowel inflammation (Crohn’s disease), or heart function (echocardiography, nuclear medicine stress test). It helps doctors monitor a condition’s status and alert them if your treatment needs adjustment.
Imaging is a cornerstone of modern medicine. It can help check the healing process of a broken bone, look for signs of breast cancer, or simply figure out why you’ve been having stomach aches. It’s all about getting the full picture of your health and ensuring you get the care you need right when you need it.
What is Radiology?
Radiology is the branch of medicine that specializes in the use of medical imaging to diagnose and treat diseases within the body. It encompasses a range of techniques that visualize the internal parts of the body, allowing doctors to see beyond what the eye can see (some forms are literally X-ray vision).
Just as photographs can capture moments in time, radiology captures images of the body’s internal state at a specific moment. These images are vital in providing a comprehensive view of your health and guiding decisions about the best path to wellness.
Who is a Radiologist?
A radiologist is a specialized medical doctor (physician) who interprets your medical images. They “read” the stories being told by your X-ray, CT scan, MRI, ultrasound, mammogram, etc. While they don’t usually operate the imaging machinery themselves (aside from fluoroscopy and interventional radiology), they work closely with the technologists who do.
Radiologists create the protocols that the technologists follow, ensuring that the images taken are of the highest quality and provide the necessary information. Radiology technologists are integral to the process.
What is a Radiology Report?
A radiology report is the radiologist’s written findings of what they saw on your medical imaging and concludes with what they think is going on. Radiology reports include the trees (each individual finding) and the forest (the big picture of what’s happening).
This report is a crucial piece of information, helping the referring physician (the doctor who ordered the image) to understand what’s happening inside your body and decide on the best course of action for your care.
Unfortunately, radiology reports are full of medical terminology and jargon, making them often difficult for most patients, sometimes even the providers, to understand.
With these insights, let’s move on to better understand the full picture (pun intended!) of your radiology report.
The Radiology Report
Without further ado, let’s take an in depth look at the radiology report.
Report Format: The Basics
Radiology reports are carefully organized to provide a clear and detailed account of the radiologic findings. Let’s go through the basic report format and cover the typical sections you’ll encounter in your report.
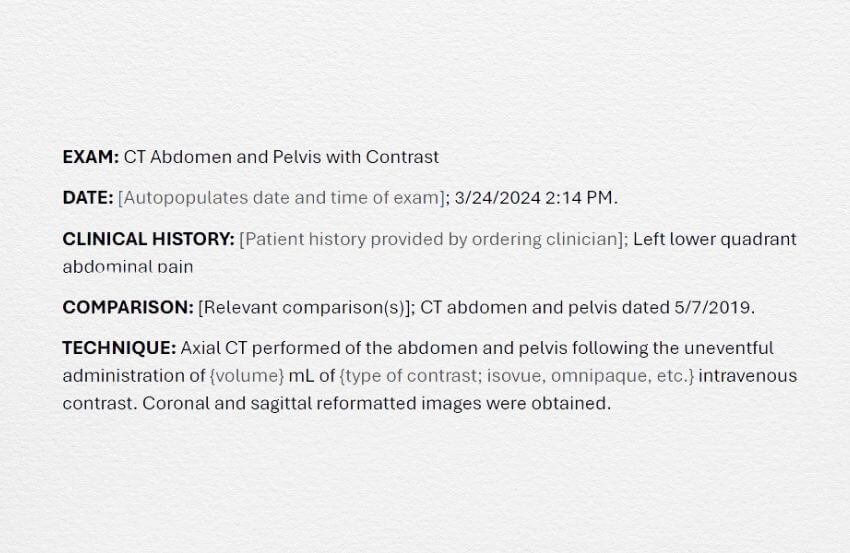
Exam
All radiology reports have an “Exam” or “Examination” header that states what the exam is and commonly the date and time the exam was performed. This is the time that the exam was done, not the time of the radiologist’s interpretation.
Clinical Information
This is where the radiologist lists any relevant information provided by your referring physician. It may include your symptoms, the specific questions your doctor wants to answer with the imaging, and any important aspects of your medical history. Think of it as the backstory that sets the stage for interpreting the images.
Note: Radiologists are not always provided with an accurate or detailed clinical history. Our wonderful technologists will frequently ask you what exam you’re having done and why. This serves multiple purposes—it confirms the correct exam is being done, the correct protocol will be followed, and that the radiologists have accurate information crucial to an accurate interpretation. It’s also important for patients to understand what they’re having done and why they’re having it done.
Comparison
In this section, the radiologist typically references any previous imaging studies you’ve had. This is like the “before” part of a “before and after;” it helps the radiologist see if there have been any changes over time. It’s a way to track the progression or improvement of a condition. It also lets the radiologist determine if something is stable over time and therefore likely “benign” (i.e., nothing to worry about).
Note: Radiologists may not have access to studies performed at different imaging centers or hospitals. Suppose the purpose of your scan is to follow up on a condition, and you have prior imaging from another site within a different health system or an unaffiliated outpatient imaging center. In that case, it’s important to request that those exams be copied onto a CD that you can bring with you to your appointment. Office or hospital staff can upload your outside studies for the radiologist to review.
Technique
You can generally ignore this part. It relates to the techniques used for the imaging procedure to acquire the images the radiologist reviews. These are a standard part of every radiologic report required for any imaging study. They may be generic and often part of a template to meet basic billing requirements.
Procedure
Interventional radiology procedures generally have a ‘procedure’ section that gives detailed descriptions of the procedure performed. The length varies with the complexity of the procedure being performed.
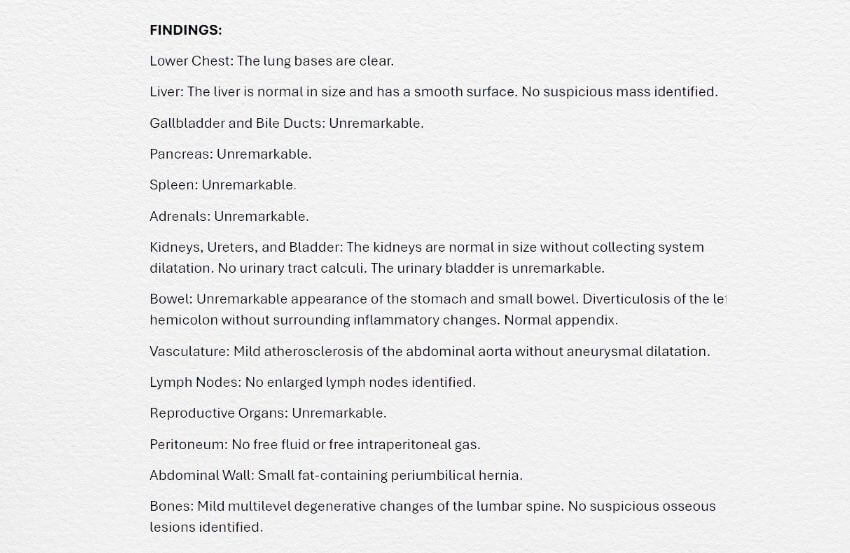
Findings
This is the “meat and potatoes” of the radiology report, where the radiologist describes what they see in the images. They’ll note the appearance of organs and tissues and point out anything abnormal. The findings are the radiologist’s observations without any interpretation—just the facts, like a list of items found by a detective on a case.
Radiologists may use standardized templates (aka structured reports) that are broken down into each organ system (e.g., liver, gallbladder, bile ducts, pancreas, etc.) and/or use standard phrases.
- CT Abdomen and Pelvis Examples: “Liver: Within normal limits.” or “Liver: The liver is normal in size and appearance. The surface contour is smooth.”
- Head CT Example: “The gray-white matter is preserved. No midline shift.”
Some radiologists prefer to “free dictate” their radiology reports, which read more like a book, a paragraph at a time. This can lead to a lot of variability. However, all reports should contain detailed descriptions of all key findings.
If a radiologist doesn’t specifically comment on something, it doesn’t mean they didn’t look at it. As radiologists, we are responsible for everything on every image. That being said, we’re not perfect (despite our best efforts).
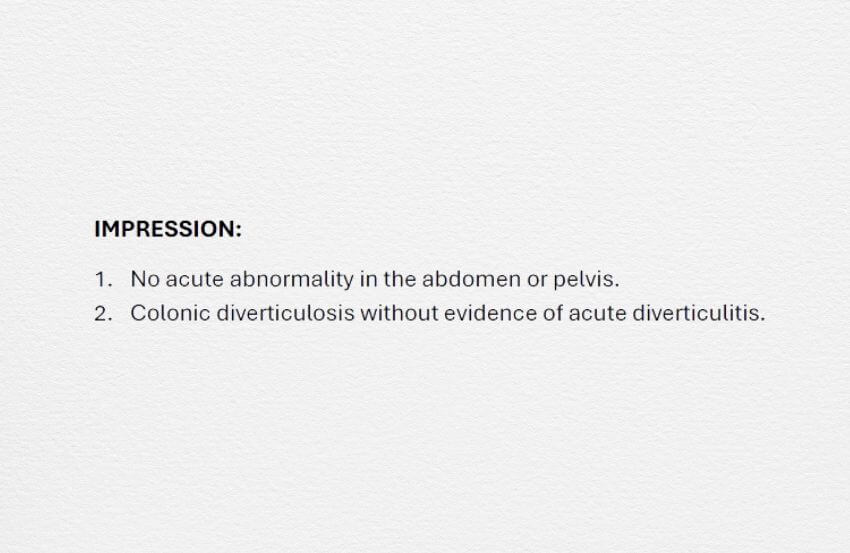
Impression
The “Impression” section is the most important part of radiology reports. It’s where the radiologist summarizes what they saw in your images, typically in order of importance, to paint an overall picture of what they think is going on. It’s a concise interpretation of the findings that can lead to actionable items for your referring provider.
The impression is where the interpreting radiologist will give or suggest a possible diagnosis (e.g., appendicitis, bowel obstruction, brain bleed, etc.) or give a differential diagnosis – a list of possible explanations to account for the findings – when they can.
It’s important to note that the radiologist interpreting your exam may not find an underlying cause for your symptoms. There may simply be no imaging findings to explain your symptoms—this is not uncommon. This doesn’t mean your symptoms aren’t real; it just means we aren’t able to see any diagnostic imaging findings that would explain them.
An impression will also include unexpected incidental findings of clinical significance – something that will require follow-up (e.g., an incidental lung nodule), further evaluation with another imaging study or lab work (e.g., an indeterminate adrenal nodule), or risk stratification (e.g., work-up for coronary artery disease).
Impressions may also include the phrase “recommend clinical correlation,” a term radiologists use to signal to your provider that we’re not sure of the significance of a finding, but the referring clinician can likely narrow it down by asking you more questions and/or doing some further testing.
The impression of your radiology report gives you the radiologist’s expert opinion of the significance of any and all findings (abnormal and normal findings) after your radiologist has taken into consideration your clinical history (symptoms and pertinent past medical history/surgeries) and compared these findings to relevant prior imaging (when available).
A great radiology report will tie all key findings together and have a clear and impactful impression.
Example Impressions:
- “Acute uncomplicated appendicitis.” – Run-of-the-mill appendicitis that can head straight to surgery (no complications are present that could delay or complicate surgery).
- “Interval decrease in size of the previously noted liver metastases, compatible with a positive response to treatment.” – A patient with metastatic cancer (cancer that has spread to other parts of the body) has had a positive response to their current therapy, meaning the current therapy regimen is working (YAY!!).
- “No acute intracranial abnormality” – Nothing concerning was found on a patient’s head CT.
- “No acute fracture or dislocation” – No broken bones or dislocated joints.
Communication
Radiologists document direct communication with referring physicians or providers for critical findings at the end of radiology reports, below the impression. These are generally urgent matters that require prompt treatment.
Radiation Dose/Exposure
While not mandated (at least not yet), some institutions may include your radiation exposure from your imaging examination. This may become required in the future as a way to keep track of your total radiation exposure and estimate future potential radiation-related risks.
Addendums
An addendum occurs when a radiologist wants to alter a radiology report after it’s been finalized. Medicine is somewhat unique in that once a document is finalized, it becomes a permanent part of the patient’s medical record and cannot be edited. This is done for patient safety, preventing providers from altering documents.
Radiology reports can, therefore, only be altered by adding to the original report in the form of an addendum. This is frequently done when an outside comparison becomes available, there is a change to the report (again, we’re not perfect despite our best efforts), additional verbiage is required for billing purposes, or we’re correcting a voice recognition error—our voice recognition software also isn’t perfect, and we aren’t expert proofreaders.
Those of us who use structured reporting may also get distracted by imaging findings and mistakenly forget to update certain parts of the report template, commonly whether or not the gallbladder, appendix, or uterus/prostate gland are present or surgically absent. If you notice this, feel free to let us know, and we’ll happily correct the report with an addendum 🙂
Preliminary and Final Reports and “Wet Reads” – What’s the Difference?
Sometimes, you might hear about ‘preliminary’ reports, ‘final’ reports, and/or “wet reads.” Here’s a quick breakdown of what these are.
A preliminary report is just that, a preliminary interpretation of the exam.
Preliminary reads are generally given by a radiology resident (a radiologist in training), an attending radiologist, or a radiologist from a contracted teleradiology group that provides evening and/or weekend coverage for some hospitals. The reports may be bare bones, only containing pertinent positive findings, or full reports, and are made available for the referring clinicians after hours.
Preliminary reports should have an obvious “preliminary report” label. Some may be very brief and even indicate “the full radiology report to follow” at the bottom of the report. Preliminary reports are frequently used for patients admitted to a hospital, referred to as “inpatients,” after hours to pass along important findings when there isn’t sufficient time for the radiologists to do a full radiology report.
The exams must later be reviewed by an attending/staff radiologist and finalized. Occasionally the attending radiologist will disagree with the preliminary interpretation (remember, we’re all human) and generally will contact the ordering provider when the change is likely to have significant clinical implications.
A final report has been reviewed by and finalized by a staff (aka attending) radiologist. This is the full radiology report that becomes a permanent piece of your medical record.
A “wet read” is a clinician’s first thoughts after taking a quick look at an exam. Radiologists and non-radiologists can both give “wet reads,” particularly when a patient’s condition necessitates urgent medical care.
Fun Fact: The term “wet read” dates back to before digital images, back when radiology films had to be developed with chemicals (similar to photography). So a “wet read” entailed looking at a radiology film hot off the press, still wet because the developing agent hadn’t fully dried.
Abnormal Findings
If you’re having an imaging examination, odds are you are experiencing some symptoms and your referring clinician is trying to identify the underlying cause/problem so they can fix or manage it. Given you feel abnormal, it’s pretty common that your radiologist identifies something abnormal to explain it.
An abnormal finding is a generic description of anything outside the realm of normal. Abnormal findings can be benign (noncancerous), malignant (cancerous), or related to another underlying disease or condition (e.g., coronary artery calcifications due to underlying coronary artery disease).
Example: Your radiologist describes an inflamed sigmoid colon diverticulum (description in findings) due to acute diverticulitis (diagnosis in impression) accounting for your left lower abdominal pain.
That being said, not finding an underlying cause may reassure that there’s nothing sinister lurking inside. While a normal exam can be reassuring, it can also be frustrating as it does not identify the cause of your symptoms.
Incidental Findings
Unrelated abnormal imaging findings, known as incidental findings, are identified in about 15-30% of radiology exams and 20-40% of CT scans (keep in mind we perform over 80 million CT scans/year in the United States alone).
Fortunately, the vast majority of incidental findings are of no significance. Unfortunately, we can’t always determine this on the exam where it’s discovered, which can lead to further studies (cost and anxiety) and potentially prolonged follow-up, biopsies, and even surgery. A very small minority of these incidental findings will turn out to be cancer and their detection can prove to be life-saving.
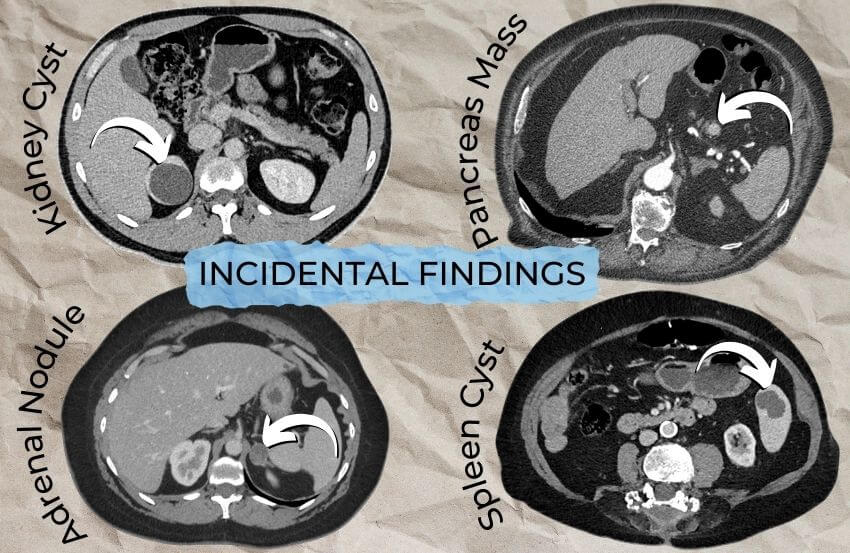
Given the high frequency of incidental findings, the American College of Radiology has developed multiple guidelines specific to various commonly encountered incidental findings. Radiology reports should include important incidental findings and appropriate follow-up recommendations (based on these guidelines) in the impression of the report.
Clinical Correlation
The human body is incredibly complex. While we may make all of the essential findings, we don’t always know the significance of the findings. There’s also some overlap of normal and abnormal conditions, which further complicates our interpretation. Radiology scanners, from x-ray to computed tomography (CT) and magnetic resonance imaging (MRI) scanners, sadly, are not crystal balls.
Radiologists are often provided with very focused clinical histories (just your symptoms, no other medical history – this is generally appropriate) and therefore will not always know or be able to determine the significance of these findings.
In these cases, where we see something abnormal or potentially abnormal and we’re not sure of the significance, we may ask your referring physicians for help with the phrase “recommend clinical correlation.”
For example, the wall of the bladder and large bowel can both be normally thickened when they’re decompressed/under distended (their walls contain muscles that may be contracting – just like your bicep will get larger when you flex) but wall thickening is also the most common finding when those same organs are infected or inflamed. Luckily, these patients will have very different clinical pictures – one will be asymptomatic and the other will likely have symptoms. This is an easy clinical question to answer – your ordering provider can just call you and ask if you’re having symptoms.
Beyond the Report
Now that you’re more familiar with your radiology report, let’s dive a little deeper.
Radiology Reporting: A Balancing Act
At our core, we radiologists are translators. We translate the imaging findings we see into purposeful prose full of detailed descriptions of relevant findings that culminate in a thoughtful, succinct impression.
Radiology reporting is an art that balances thoroughness with clarity. All relevant findings, including pertinent negatives (e.g., in cases of pulmonary emboli [blood clots in the lung] we comment on the presence or absence of right heart strain [increased back pressure on the heart from a large clot burden] that may require more aggressive treatment), must be described and transformed into a meaningful and understandable impression.
Radiology reports may have an overwhelming number of imaging findings that need to be converted into a clear and concise impression that is easy to understand for your referring physician. The impression can be thought of as a “Cliff’s notes” version of the report, containing all of the pertinent information in condensed form.
I personally put anything of clinical significance in my impressions. If it’s not in the impression, it can likely be ignored.
Dissecting the Report
Understanding the anatomy of the report is a good start, but what, as a patient, should you expect to take away from it?
As mentioned above, imaging reports are geared toward referring physicians, not patients. They tend to be full of medical terminology and can be pretty confusing, even to a referring physician (to be a good radiologist, we have to know a lot about a lot, which includes many uncommon and rare pathologic conditions).
Google will only get you so far and can either further confuse you or send you down rabbit holes, some of which can lead to anxiety (I don’t know about you, but I have a tendency to overly focus on the worst possible scenario). Luckily, you have a healthcare team that also has a copy of your report and should be able to answer (or find answers to) any questions you may have.
Focus on the impression of the report. The impression should provide an answer to the clinical question that lead to the imaging examination or conclude the exam is normal, has no acute abnormality, or no findings identified to explain you symptoms.
If you find something confusing or feel there’s too much medical terminology, write down a list of questions to ask your provider.
Radiology Reports: Impact on Patient Care
While radiology somewhat flies under the radar, it is a cornerstone of medicine. Radiologists are diagnosticians and problem solvers. We combine your symptoms and clinical history with imaging findings to solve the clinical question that lead to the imaging examination.
In fact, radiology reports are frequently where many medical conditions are first diagnosed. Cancers are discovered, staged, restaged, and surveilled. Medical and surgical emergencies are identified and rapidly communicated to the healthcare team to expedite patient care.
Radiology reports directly and indirectly impact patient management on a daily basis.
Why It’s Important for You to Understand Your Radiology Report
Patient access to medical records has drastically improved now that many hospitals and clinics offer patients direct access to their medical records through an online patient portal. This is a secure website where your health information is kept, from your medical history and clinic notes to your laboratory and radiology results.
As patients, you can now log into your patient portal and view your reports (sometimes even before your primary care physicians and specialists!). But with great access comes great responsibility 😉
While your healthcare provider (and the entire healthcare team) prioritizes your health and well-being, it’s your health at the end of the day. No one should be a bigger advocate for your health than you.
Knowledge is power. Understanding your radiology report can empower you to be a more active participant in your healthcare. When you understand your health and any underlying conditions you may have, you’re able to make more informed decisions and take ownership of your health. Life is too short to take your health and well-being for granted.
How to Best Advocate for Yourself as a Patient
Navigating your healthcare can be complex, but being your own advocate is a powerful step toward getting the best care. When it comes to radiology, it’s essential to remember that radiologists, as skilled as we are, aren’t wizards. We rely heavily on the clinical history you provide to give the most accurate interpretation of your imaging.
Provide a Detailed Clinical History
The importance of providing a good clinical history to the radiologist cannot be overstated. A thorough clinical history is the map that guides the radiologist through the terrain of your imaging.
If your situation isn’t communicated fully – say, the radiologist only knows you have “abdominal pain” without the detail of that unfortunate encounter with your kitchen table or that it started in your belly button area, moved to your right lower abdomen, and was associated with nausea and a loss of appetite (classic history for acute appendicitis) – we’re at a disadvantage.
Different conditions can appear similar on scans, so without a clear history, our ability as radiologists to pinpoint the underlying issue(s) can be like looking for a needle in a haystack. An accurate and detailed history is our metal detector. Ignorance is not always bliss. In medicine, ignorance is frequently dangerous.
The more specific you are about your symptoms and how they came to be, the better radiologists can navigate the images and come up with an accurate diagnosis and helpful report.
Note: Healthcare providers are overworked and frequently have to see too many patients in too little time. Typing in a complete and thorough history can be time-consuming, and providers may opt to select from a list of generic symptoms and/or diagnosis codes to save time. However, an inadequate history can negatively impact the radiologist’s interpretation (the results of your radiology report), and providers should make providing a useful clinical history a priority.
Ensure Accurate Information Transfer
Take the initiative to ensure that your healthcare provider has a complete picture of your clinical situation and shares it with the radiology team. Don’t hesitate to clarify any details you feel might have been overlooked. It’s better to over-communicate than to (incorrectly) assume your radiologist has information they don’t actually possess. As a patient, you can share this information with the technologist taking your images, who can then provide the radiologist with a more detailed and accurate history.
We frequently only have access to the clinical information that’s provided, so ensure your doctor includes relevant details, including more than just “pain.” You can check the “Clinical History” section to confirm an accurate history was provided.
Read the Radiology Report
Receiving your radiology report can often feel like you’re about to read a technical manual for an appliance – confusing and not always straightforward.
However, if you’ve read this far, you should have a basic foundational understanding of the radiology report. Focus on the impression. Take note of anything you find confusing so you can ask your provider for clarification.

Review the Clinical Information
The first step is to review the clinical information. This section should mirror the symptoms and history you discussed with your doctor.
If there’s a mismatch or something crucial is missing – for instance, if the report only mentions “pain” but doesn’t include a specific location, recent injury, or other associated symptoms – it’s important to know that your radiologist may not have had the full story when interpreting your images.
Feel free to notify your healthcare provider if you’re concerned the history they provided didn’t accurately reflect your symptoms. The details can change the interpreting radiologist’s approach and focus, potentially altering the findings and impression.
Understand the Findings
The findings are the radiologist’s detailed observations of the images. While this section may contain medical terminology, don’t be discouraged. It’s intended to capture anything out of the ordinary or worthy of note that the radiologist sees on your scans.
Don’t get bogged down by the findings. If there’s a section to skip, this is it. All of the important and actionable items will be in the impression.
Reflect on the Impression
The impression is the most essential part of your report – this is where your time is best spent. Here, the radiologist distills their observations into a coherent summary and relates them to possible diagnoses or follow-up actions.
Read this section carefully. Does it make sense in the context of what you’re experiencing? Does it address the concerns that led to the imaging in the first place?
Ask Questions
Ask questions if there’s anything you don’t understand or seems incomplete. It’s your right to have a clear understanding of your health information. Your healthcare team expects and welcomes your inquiries – they’re a sign that you’re engaged and taking an active role in your health management.
By reading and understanding your radiology report, you’re not just passively receiving information; you’re checking it for accuracy, gaining insight into your health, and ensuring that your care is on the right track. Your proactive participation is vital to the care process, leading to a more personalized and effective treatment plan and a healthier you.
Final Thoughts
Your radiology report is more than just medical jargon on a piece of paper (though it’s definitely also that 😉); it’s a snapshot of your current health and a roadmap for future care. Understanding it empowers you to take an active role in your health decisions.
So, next time you’re handed a radiology report or are checking one on your patient portal, take a moment to read it over. Ask questions if you need to—your healthcare team is there to help you make sense of it all.
Remember, you’re the most important member of your healthcare team. Stay curious, stay informed, and stay healthy!
If you enjoyed this article and would like to see more like it, consider supporting my work with a virtual coffee! ☕